From Facebook:
 (Yes, I went there.) We are sleepless in Seattle over Idan’s latest chimerism test results. Once again, the numbers are not where we hoped they’d be, and, worse yet, are indicating that the graft is slipping even further. Idan’s T-cell count remained low, nudging up only a few percentage points from 7% to 12% donor from the DLI. This would have been fine if not for the fact that his myeloid cell line, which had been at or near 100% from the beginning, has slipped down to 83% donor.
(Yes, I went there.) We are sleepless in Seattle over Idan’s latest chimerism test results. Once again, the numbers are not where we hoped they’d be, and, worse yet, are indicating that the graft is slipping even further. Idan’s T-cell count remained low, nudging up only a few percentage points from 7% to 12% donor from the DLI. This would have been fine if not for the fact that his myeloid cell line, which had been at or near 100% from the beginning, has slipped down to 83% donor.
There are two possibilities for the slip down. The first and more likely is that Idan is rejecting the graft (probably because he does not have a substantial number of donor T-cells). The second possibility is that the myeloid cells are just fluctuating and will stabilize at a high number. We are redoing the chimerism test next week to see if it continues to drop. If so, we know that we are likely facing rejection. Obviously, we are hoping and praying for the graft to hold tight and for the T-cells to continue increasing. We are planning for a second DLI on January 27th, but that plan may change depending on the test results next week.
Without speculating too far into the future, should Idan reject the graft, we will have to gear up for battle again. There is some new research indicating that Idan’s disease makes him susceptible to an even greater array of opportunistic infections than initially thought, and that the CD40 ligand protein is implicated in more areas of the immune system than just the creation of IgGs (hence why IgG replacement therapy is not sufficient to protect Idan).
A second transplant comes with even more risk than the first one and is a very scary thought, so we are praying that we do not have to go down that road. That said, we think back to our initial reasons for choosing Seattle and feel comforted knowing that Idan is still strong and did very well throughout the transplant. There are definitely scenarios far worse than rejection. No matter what the next chimerism results show, we have no regrets.
We are blessed with a child that fills our heart with joy and laughter, and allows us to forget our fears and worries. We hope that we can do the same for him by staying strong, happy and optimistic – but prepared to go back into battle if necessary.
Idan being playfull while trying to avoid bath time
It’s been a long week. It started with yet another medical mystery. On Tuesday, we took Idan to the hospital to test his swallowing ability. Since his first hospitalization in April, he’s had random choking fits while eating or playing that have gotten worse since transplant. We initially thought it was acid reflux, but decided to take a closer look to make sure bacteria wasn’t quietly entering his lungs with these fits. It turns out, Idan does have a problem swallowing liquids. He is having some mild aspiration, which is concerning enough that we are now thickening all of Idan’s drinks to make sure he doesn’t choke. It doesn’t seem to be connected to the transplant since it started after his intubation last April, but it’s not clear what is causing this problem. In any event, we are hoping Idan grows out of it.

Getting his X-rays
Shortly after the swallowing test, Akiva felt a scratch in his throat, and we had to separate him from Idan until we knew for sure he did not have a cold or, if he did, he was free of symptoms for at least 48 hours. Thankfully, the scratch in his throat went away, but the scare meant Idan and I were on our own for two days. Ever since we came to Seattle, Akiva and I have worked in unison to care for Idan as the three of us hunkered down for his bone marrow transplant. It hadn’t quite dawned on us just how much care and energy our situation necessitates until I was without my partner.
Our routine starts at 7:00 a.m., with Idan’s first medication of the day – tacrolimus. This must be given every 8 hours. Idan is usually up by then, so we give it to him right on time. Then, his central line must be flushed. His central line splits into two lines. Both lines must be flushed once a day. This requires first cleaning the two lines with an alcohol swab, then pushing a saline and then heprin syringe into each line. After breakfast, we take Idan’s temperature, and then measure out and prepare his 6 or 7 oral medications (depending on the day of the week), and give them to him a ½ ML at a time (more syringes). After oral meds, we can play, go outside, and do “normal” activities until it’s time to leave for the clinic. We go to the clinic two or three afternoons a week for Idan’s regular exams, blood draws, infusions, to pick up new meds, and to talk to the pharmacist about any changes to the meds. These visits can last anywhere from 1 ½ to 3 hours, depending on what’s lined up for the day. We usually have to pack his 3:00 dose of tacrolimus to make sure he gets it on time. The clinic visit often ends with a cranky child who, although loves visiting all his friends, gets pretty frustrated that he can’t crawl or walk around.
After clinic, we give Idan more medicine for his acid reflux, and then we have Facetime/Skype chats with family on the East Coast over dinner. After dinner, Idan gets 5-6 more oral medications. Then we can get Idan ready for his bath. Before the bath begins, the entire tub must be thoroughly cleaned, a few fresh towels and washcloths are set aside in a clean area, and Idan’s dressing must be covered. Small pieces of film are wrapped around the ends of his line to prevent moisture from coming in, and a piece of gauze is placed on some Press N’Seal wrap to cover his entire dressing. Idan’s entire chest and stomach are covered, and he gets a bath standing up – no splashing in water for him. Before he goes to bed, he needs another bottle to meet his fluid goals for the day, so we put on some Curious George while he finishes up. We do one last temperature check before he is carried into the bedroom. One of us will put Idan to sleep, and the other works on cleaning the rest of the house so it is ready for Idan in the morning. Our night ends at 11, when we give Idan his last dose of tacrolimus for the day, trying not to wake him.
Imagine doing all of the above with an active toddler who weighs over 30 lbs, and on only a few hours of uninterrupted sleep! It was a happy reunion when Akiva was able to join us again. During his period of isolation, Akiva finally got a chance to deal with our insurance and bills that are starting to come in – and finally got a haircut! I learned how to do all of the above with no help (although Idan does enjoy helping me wrap his central line before bath), and in spite of it all, had a ton of fun with the cutie. So, not all bad…
Next week is a very busy week. We have the next chimerism test on Monday morning, bright and early. The rest of the day/week will be filled with a repeat of all the tests that were done pre-transplant for the post-transplant evaluation typically done between Day 85-100. These days don’t matter nearly as much for us given Idan’s difficulty engrafting on his T-Cell line, but it is important to know how well his organs have withstood the chemo, etc.
We will have lots to report in a week, so stay tuned…
From Facebook: Idan went out yesterday for a short walk around our block. While his immune system is still very much compromised, we need to mostly avoid children and people. Mid-day on a cold day seamed like the best time to test out his new walking skills:
 Hyper IGM, bone marrow transplant, immunodeficiencies, what does this all mean and why are we doing all this to our son Idan? For those of you still trying to make sense of the whole process, I am going to try and simplify it so that it is easier to follow.
Hyper IGM, bone marrow transplant, immunodeficiencies, what does this all mean and why are we doing all this to our son Idan? For those of you still trying to make sense of the whole process, I am going to try and simplify it so that it is easier to follow.
What is X-Linked Hyper IGM?
Our son Idan was born with a genetic mutation passed along on his X Chromosome. The syndrome itself almost always only affects boys as girls have two X’s and are mostly just carriers. Since it never appeared in our family before, we had no way of knowing Idan had this until he got sick in April. Hyper IGM is so rare (2 in 1,000,000) that it is never something that is tested for (and most doctors probably never even heard of it).
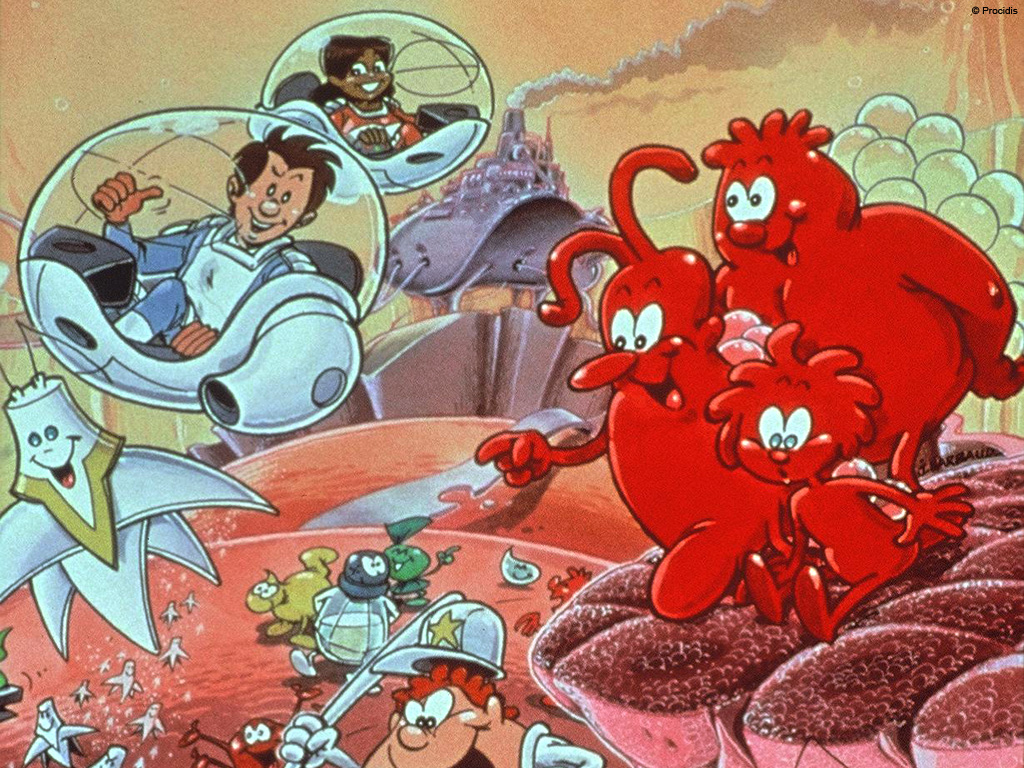
So how does it affect Idan? Basically the gene mutation means that he is missing a protein that his T-Cells need to produce (called CD40 Ligand) that is necessary to produce Antibodies, or immunoglobulins. This protein is also used by the T-Cells to communicate (AKA tango with) with the B-Cells and allow them to do their job as needed. This leaves a huge hole in his immune system. Imagine an army with lots of foot soldiers (T-cells) and Special Forces (Immunoglobulins) constantly at battle with the world around us. This army keeps us all safe on a daily basis, and when we encounter viruses or bacteria that the foot soldiers cannot not fight off, the special forces take over. Idan has no ability to create special forces at all, so he cannot recognize or destroy any viruses (think flu, cold, mono, herpes, etc.) so those can kill him. He also has lots of T-Cells that do not know the basics of fighting because the B-Cells cannot give them proper instructions. Therefore, he is susceptible to many opportunistic infections (like the PCP/PJP that almost killed him in April) that the rest of us just fight off without even feeling sick.
What are the dangers of Hyper IGM?
First, recurrent infections can lead to major organ damage. Idan’s lungs were in very bad shape after beating the pneumonia back in April. As time goes by many Hyper IGM kids have orgran damage to the lungs and liver from these infections. Second, opportunistic infections such as cryptosporidium, a parasite found in water, can kill Hyper IGM patients as there is no cure for cryptosporidium without a functioning immune system. Lastly, cancer, malignancies and liver and central nervous system diseases. As time goes by there are higher risks of all these, leading to a median age of 24 for Hyper IGM patients. Our immune system is constantly fighting off cancers before they even become an issue and our son’s immune system cannot do that.
So what can be done?
In the short term we have been treating Idan with immunoglobulin replacement therapy. These are the weekly infusions of IGG’s which is one of the 4 types of antibodies he is missing, and the only ones medicine knows how to replace. This, coupled with major lifestyle changes (like isolation, bottled water, etc.) has kept Idan safe since April. Some Hyper IGM patents can live for many years this way, but since Idan’s mutation is the most severe form (i.e., he expresses no CD40L at all), the odds of this being enough are against him. The only known possible cure is a Bone Marrow Transplant which essentially would replace his entire army with a donor’s army that works properly. But this is a complicated and risky process with high risks and no guarantees.
So What Is a Bone Marrow Transplant (BMT)?
Currently, there is no way to fix the gene mutation that causes Hyper IGM, but there is a way of replacing the bone marrow and giving Idan a new immune system. One can look at the bone marrow as the army base that the immune system (as well as the blood) is created and trained in. The idea is, if Idan’s b-cells cannot produce the protein he needs, lets give him a new army base, with soldiers that know what they are doing. But it is not that simple:
1) Currently the army base in his body is filled with soldiers (even if they’re not too smart), so there is no vacancy for him to host someone else’s army.
2) Idan’s body (AKA, the equipment, building and land that needs protection) is a perfect match with his current army, and no other army (AKA the donor’s bone marrow) is going to know how to work it in the same way.
3) Any gap in the protection that his army is giving him (albeit a lazy one) will open up his body to infections.
4) In order to create a vacancy in his army base so that a new army can move in, the old one needs to be eliminated entirely. The way they do this is with chemotherapy, which has the nasty side effect of destroying the bone marrow, and in our case we want that. However, that process comes with its own risks of toxicity to the body.
With all the risks involved Amanda and I decided that BMT is the way to go. BMT will give Idan the best chance at a long and healthy life. We did a lot of homework and spoke to dozens of bone marrow teams around the world. We decided on Seattle because of the new type of chemo drug they are using (Treosulfan) that is less toxic than others. If all we need is to clear the army base from soldiers why bomb random cities and cause damage to the whole land?
How will this cure Idan?
First they will use chemo and ATG to eliminate his bone marrow and suppress his immune system. This is what we are doing from Day -6 to Day -1. We then give Idan a day of rest while the chemo in his system continues to clear out all the soldiers from his army bases (including the civilian side of his bone marrow that produces red blood cells). On Day 0 the transplant date, we will infuse Idan with the donor’s army. His army has been found to be a 10/10 match to Idan’s. While this is great news, it is not the whole picture. This new army is not really going to understand how to relate to all of Idan’s body parts, and will most likely still want to attack some of it (this is called Graft ss Host disease, and it happens with 70% of the transplants from unrelated donors like Idan’s). For this reason they use the ATG, and the other immunosuppressants to allow the new army to come into the empty base, but forces it to unpack, train, and start patrolling very very slowly. Giving the new army more time to get adjusted to Idan’s body is a delicate balancing act that will happen over the next year. Since they are letting the bone marrow come in and start working very slowly there is a longer time where Idan is lacking any working immune system and will be kept in isolation as well as be given drugs to protect him.
So what is next?
Day -6 to day 0 we are clearing his bone marrow and making room. On Day 0 he gets the transplant, and we start counting days until the bone marrow travels to the base and starts setting up shop. We hope to hear around Day 22 that they have reached the base and that would be engraftment. We will then wait until we see his counts go up. The first type of soldier to come back (or, better put, to “grow”) is his neutrophils (which work fine now, but we have to get rid of them with the rest of the army) and they will wait until that level is good enough to get released to isolation at our apartment. This will happen between day 30 and 50 and then we will count to day 100 before they might let us go back to NYC. From then on and until around 2 years post transplant Idan will still have a weak immune system. Our hope is that around one year post-BMT, his new army will be strong enough and acclimated to his body to start reducing the supplemental protections we are giving him. Along the way there are going to be many scary events but we and the medical team will deal with them as they come up.
In a few years, when Idan can go to nursery school, play with other kids, take swimming lessons, play in the park and ride the swings all with the protection of his donor’s army, we will know we did the right thing to ensure Idan has a normal, healthy and happy life.

Importantly, Dr. Buckley, who has seen Hyper IgM patients for the past 40 years and has seen the entire spectrum of how these individuals were affected by the disorder, both for those who opted for transplant and those for whom transplant was not an option, recommends this: Do the transplant as soon as you can with the institution that has the most experience. Idan is the “picture of health” right now, and thus has the best chance of survival and CURE.
So we have only started our journey, but agree that we need to do this once and do it right. This means visiting all the experts and hearing how they plan on reducing the risk. If it were your child, wouldn’t you go to the end of the earth, too?
Now, for our goal. According to materials provided by Duke, the average cost for families across the country to undergo a transplant is approximately $650,000 for the first year. We hope this is a high estimate in our case, where we have insurance that will cover a large portion of the medical expenses of transplant. However, our insurance does not cover IVIG, a very costly treatment Idan will need frequently for the year during and post transplant. Because this is not covered, we will likely need to pay for private insurance, but we understand there is no guarantee we will be able to purchase insurance in such a short time frame that also covers IVIG and also does not charge us a very high premium because of Idan’s condition. Regardless, we have estimated our expenses to range from $250,000 to $350,000, which is why we’ve raised our goal. We have not included in our goal the other non-medical expenses such as the visits to doctors across the country, loss of income for six months or more, and relocating expenses.
We hope you will continue to share Idan’s story, email your contact lists, and post on your facebook pages and twitter so that we may meet our goal, and, more importantly, be connected with any other experts (be they doctors or researchers) that can help us reduce Idan’s risk so that we can do this once and do it right.
Love and best wishes to all,
Akiva, Amanda & Idan

 June 9th Update: dan update: We saw the pulmonologist last week and he believes Idan’s lungs are doing very well and should be strong enough for transplant. This is great news, and should allow us to move forward quickly once we choose a doctor/hospital. We are getting ready for a trip to Duke to visit one of the expert transplant doctors for Hyper IgM and other immune deficiencies. Wish us luck!
June 9th Update: dan update: We saw the pulmonologist last week and he believes Idan’s lungs are doing very well and should be strong enough for transplant. This is great news, and should allow us to move forward quickly once we choose a doctor/hospital. We are getting ready for a trip to Duke to visit one of the expert transplant doctors for Hyper IgM and other immune deficiencies. Wish us luck!
Fundraising update: With your help, we’ve raised almost $40,000 – nearly half of our goal – in only a few days! Idan’s story has been read by over 1,000 people, 261 generously donated, and hundreds more have shared Idan’s story through Facebook, email, and Twitter! Through your efforts, we’ve even been put in touch with another doctor who has performed a successful Hyper IgM transplant. Thank you so much!

You all know our son Idan, and many of you have followed his adventures on Facebook. Idan now needs your help! Last month, after a 21 day stay in the ICU, Idan was diagnosed with Hyper IgM, a very rare life-threatening genetic disorder that plagues his immune system. We need your help, so he can live a full, long and healthy life: Please see here:https://www.youcaring.com/fundraiseforidan and feel free to Like, Share and pass along. More details and updates to follow. See here for original Facebook post.